
Why Chronic Low-Grade Inflammation Is Silently Damaging Your Arteries Right Now
Why Chronic Low-Grade Inflammation Is Silently Damaging Your Arteries Right Now
You feel fine. Your last checkup came back clean. But inside your arteries, a slow, invisible process may have been building for years.
Chronic low-grade inflammation is different from the kind you notice. When you sprain an ankle, the swelling and heat you feel is acute inflammation — your immune system doing its job. It shows up, does the work, and settles down.
Chronic low-grade inflammation doesn’t do that. It stays. The immune system remains in a low-level activated state, producing a steady stream of inflammatory compounds called cytokines. You don’t feel it. But your arterial walls do.
What Does Chronic Inflammation Actually Do to Your Arteries?
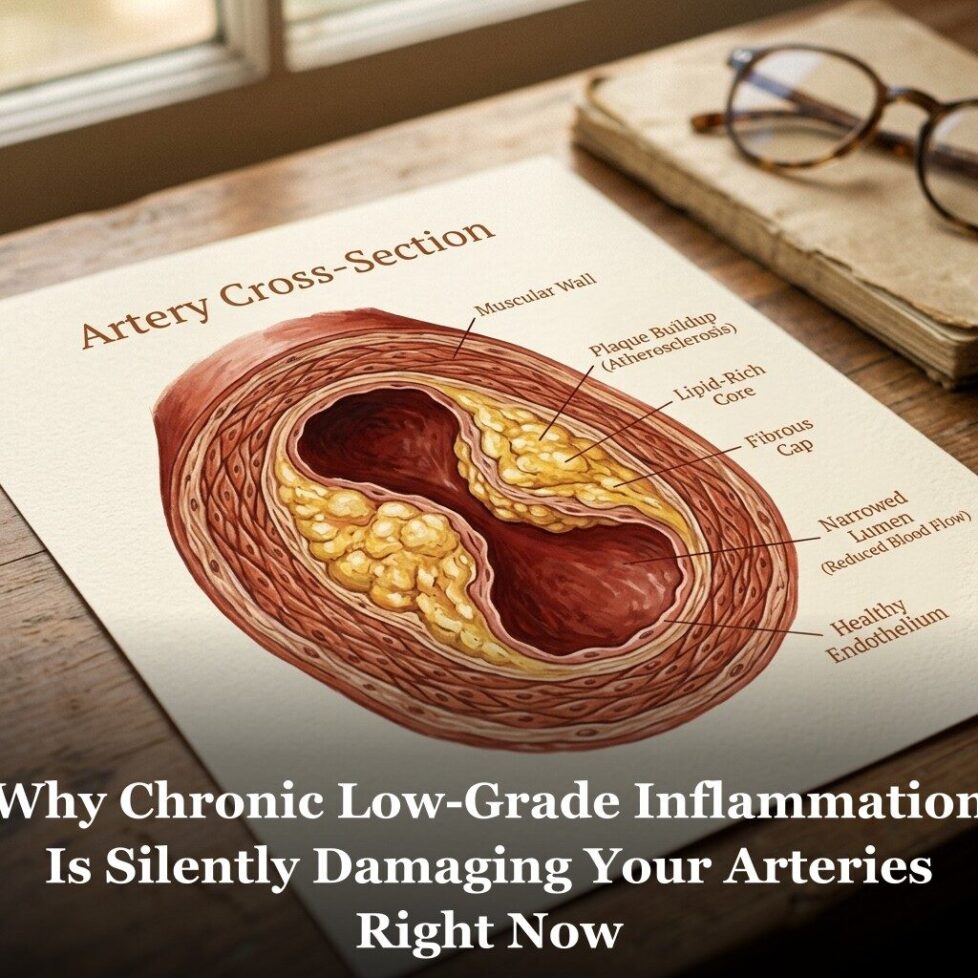
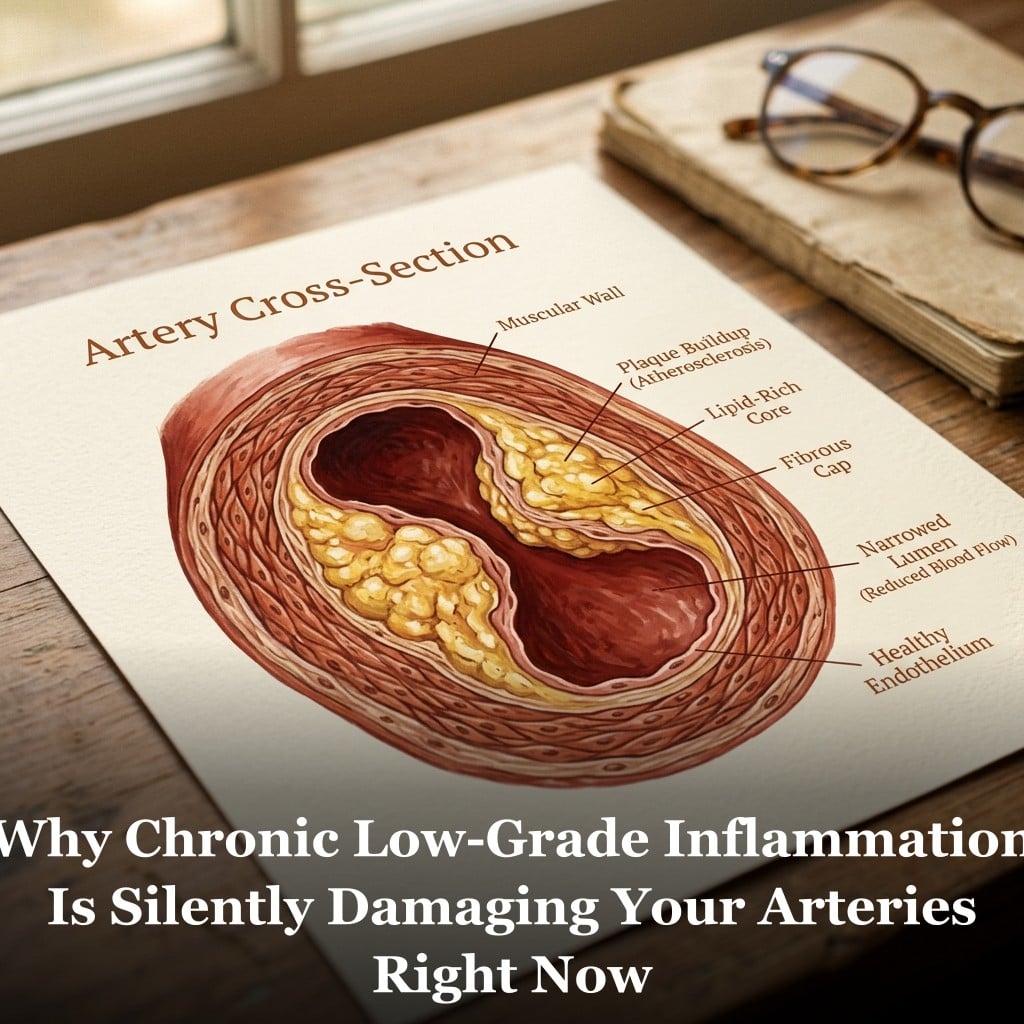
The inner lining of your arteries, called the endothelium, is just one cell layer thick. It controls what passes from your blood into the arterial wall. When it’s healthy, it does this well. When inflammation is chronically present, that lining becomes compromised.
Here’s what research has found happens next.
Inflammatory compounds cause endothelial cells to produce less nitric oxide. Nitric oxide helps arteries stay flexible and supports healthy blood flow. When nitric oxide production drops, arteries become stiffer and less responsive. This process is called endothelial dysfunction, and it’s considered an early sign of cardiovascular stress. You can read more about how this connects to arterial stiffness and silent arterial damage.
At the same time, the compromised lining becomes more permeable. LDL particles can slip into the arterial wall more easily. Once inside, they get oxidized by the inflammatory environment. Immune cells called macrophages rush in to clean them up. But when there’s too much oxidized LDL, the macrophages can’t keep up. They get overwhelmed, die in place, and form what researchers call foam cells. These accumulate into early arterial plaque.
There’s another problem that gets less attention: plaque stability. Not all arterial plaque is equally dangerous. Stable plaque has a thick fibrous cap. Unstable plaque has a thin cap and a soft, lipid-rich core. When chronic inflammation is present, it activates enzymes called matrix metalloproteinases that break down that fibrous cap. Unstable plaque is more prone to rupture, and a ruptured plaque is what triggers most heart attacks and strokes.
So chronic inflammation isn’t just involved in building plaque. It may affect how dangerous that plaque is once it forms. This connects directly to the broader framework of cardiovascular risk factors that most people have never had explained to them.
What Causes Chronic Low-Grade Inflammation?
Chronic inflammation doesn’t usually come from one thing. It builds from a combination of factors, many of them common in modern life.
Excess visceral fat. Fat stored around the organs acts as active inflammatory tissue. It secretes cytokines continuously. Even people at a normal body weight can carry too much visceral fat, which is why waist circumference matters more than the scale for cardiovascular risk assessment.
Poor diet patterns. Ultra-processed foods, refined vegetable oils high in omega-6 fatty acids, and added sugar have all been studied in connection with elevated inflammatory markers. Some trigger inflammatory signaling directly. Others alter the gut microbiome in ways that increase intestinal permeability, allowing bacterial compounds into the bloodstream and activating immune responses.
Chronic stress. Psychological stress keeps the body’s stress response system active. Cortisol is designed to be a short-term hormone. When it stays elevated, it can suppress certain immune functions while ramping up others, including those involved in vascular inflammation.
Disrupted sleep. Poor sleep quality and short sleep duration are consistently associated with elevated CRP and interleukin-6, two markers used to measure systemic inflammation. The connection runs both ways: inflammation can disrupt sleep, and disrupted sleep increases inflammation.
Smoking and air pollution. Both introduce oxidative compounds that directly damage the endothelium and activate inflammatory pathways. Former smokers can carry elevated inflammatory burden for years after quitting.
Insulin resistance. When cells stop responding to insulin properly, blood sugar stays elevated after meals. The resulting oxidative stress and elevated glucose both activate inflammatory signaling. Many cardiologists now consider insulin resistance a major upstream driver of cardiovascular inflammation.
What Does Research Point to for Diet and Lifestyle?
The good news is that most of these drivers respond to behavior. Chronic low-grade inflammation is not fixed. The body’s inflammatory state is constantly being shaped by inputs.
Research on dietary patterns consistently finds that a Mediterranean-style diet is associated with lower inflammatory markers. The core features are straightforward: more vegetables, fruits, legumes, fish, and olive oil; less refined grain, processed meat, and added sugar. The omega-3 fatty acids in fatty fish, in particular, have been studied extensively for their relationship to inflammatory pathways. You can go deeper on this with the article on nitric oxide and cardiovascular health.
Physical activity is one of the most reliably anti-inflammatory interventions in the research literature. Moderate aerobic exercise done consistently appears to reduce circulating inflammatory markers. Researchers believe this happens partly through improved body composition, partly through direct metabolic effects on immune function.
Weight loss, especially reduction of visceral fat, has a measurable effect on CRP levels. Even modest reductions can shift the inflammatory load meaningfully.
Sleep quality matters more than most people give it credit for. Poor sleep isn’t just a lifestyle complaint. It has measurable effects on the inflammatory and metabolic systems that bear directly on heart health.
Certain nutrients have been studied for their relationship to inflammatory pathways. Omega-3 fatty acids, magnesium, polyphenols from berries and olive oil, and curcumin from turmeric are among the most researched. A diet rich in plant compounds and omega-3 fats tends to be associated with lower inflammatory burden than one high in refined foods and omega-6 oils. Magnesium deficiency in particular has been studied in connection with both inflammation and blood pressure regulation.
Inflammation is also one reason HDL cholesterol’s protective role is more complex than most people realize. HDL carries anti-inflammatory properties. When inflammation is chronically elevated, HDL function is often compromised even when HDL levels look normal on a lab report.

Frequently Asked Questions
How do I know if I have chronic low-grade inflammation?
You can’t tell from symptoms alone. A high-sensitivity CRP (hs-CRP) blood test is the most commonly used clinical marker. It’s not part of a standard panel, but you can ask your doctor to add it. Levels below 1.0 mg/L are considered low risk; 1.0 to 3.0 is intermediate; above 3.0 is associated with higher cardiovascular risk. Fibrinogen and homocysteine are two additional markers some cardiologists use.
Is CRP the same as inflammation?
CRP is a marker, not inflammation itself. Your liver produces CRP in response to inflammatory signaling from cytokines. Elevated CRP tells you inflammatory signaling is present somewhere in the body, but it doesn’t pinpoint the source. It’s useful as a general signal of systemic inflammatory burden.
Can arterial inflammation improve over time?
Research suggests that chronic vascular inflammation responds to the same inputs that created it. Studies on dietary change, exercise, weight loss, and smoking cessation all show measurable effects on CRP and other inflammatory markers. The body’s inflammatory state is not fixed. Changes in diet and lifestyle can shift it, though the timeline and extent vary by individual.
Does inflammation cause elevated blood pressure or is it the other way around?
The relationship appears to run both ways. Inflammation can impair endothelial function, which affects how arteries regulate blood flow and pressure. Elevated blood pressure also creates mechanical stress on the arterial wall that can trigger inflammatory responses. Researchers generally view them as co-occurring parts of the same cardiovascular risk cascade rather than a simple cause-and-effect chain.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
Get the Free Book →* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.