
What Is Metabolic Syndrome and Why It Multiplies Your Heart Risk
What Is Metabolic Syndrome and Why It Multiplies Your Heart Risk
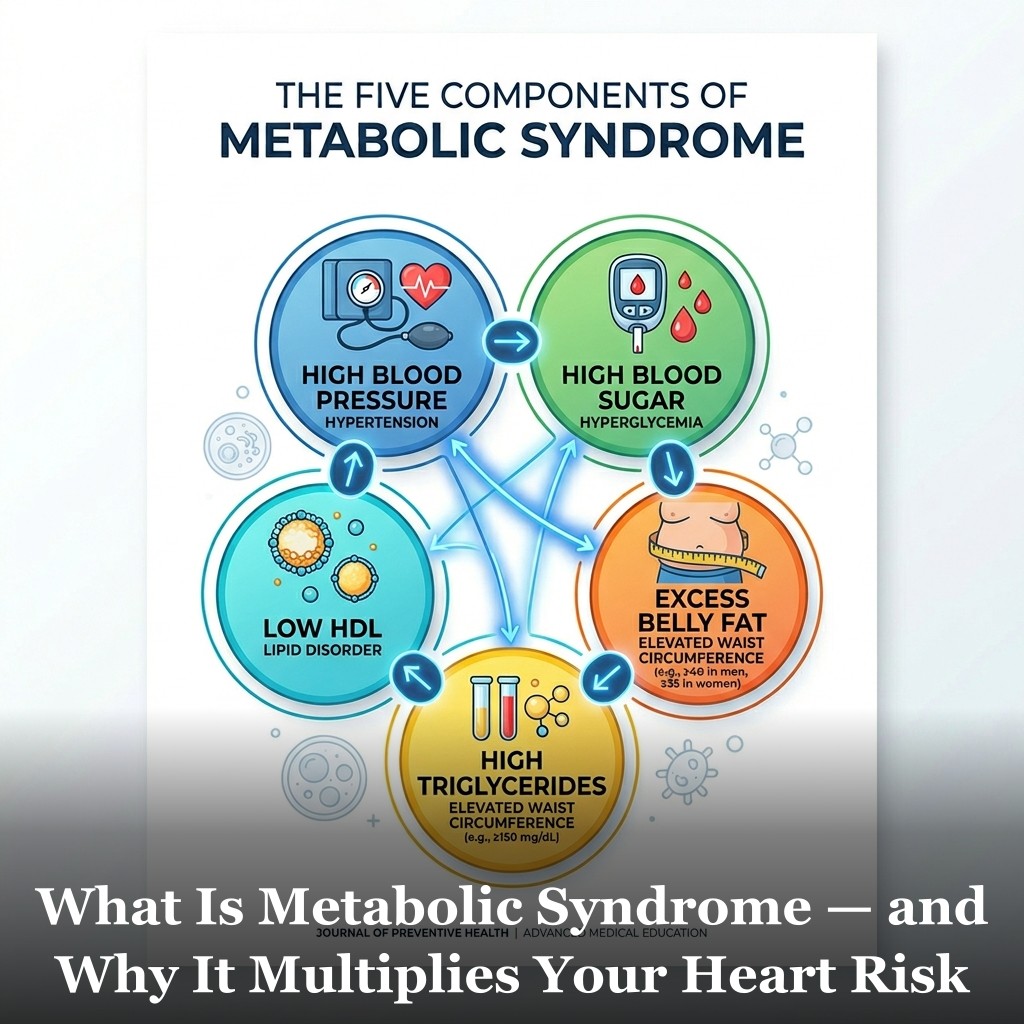
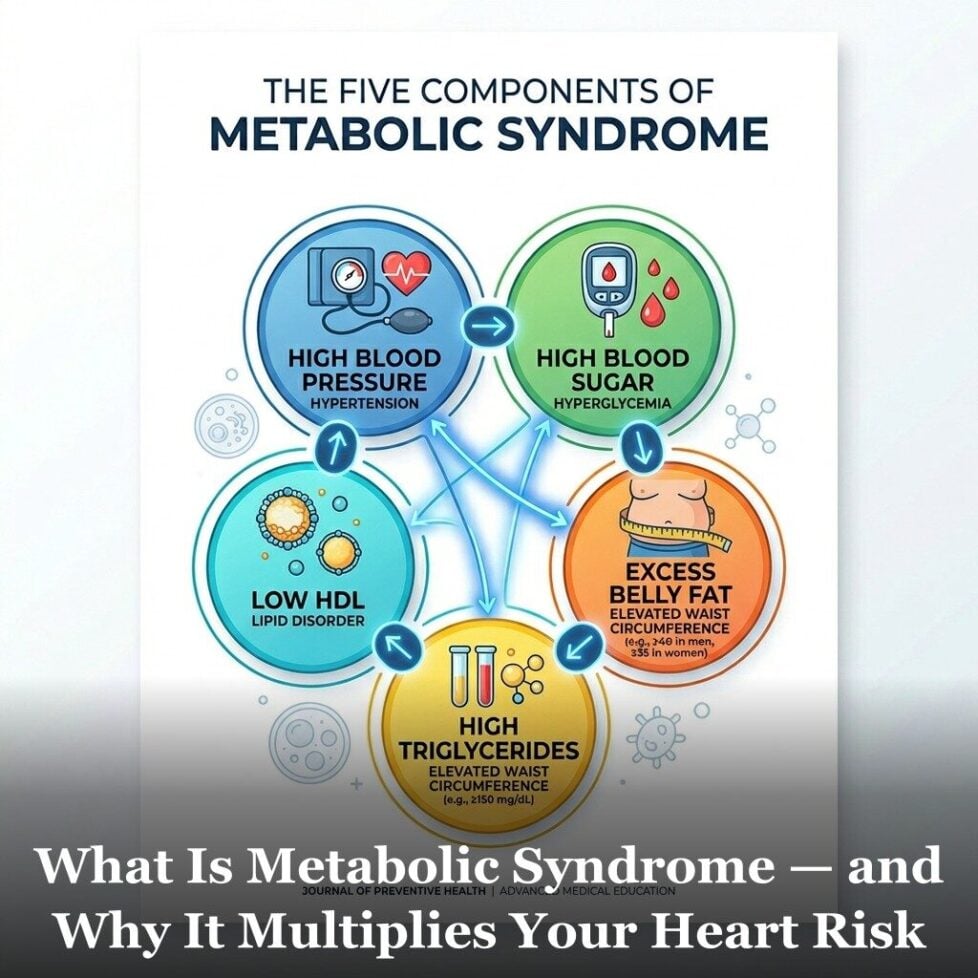
Metabolic syndrome isn’t a disease in the traditional sense. It’s a cluster. Five specific risk factors tend to occur together, and when three or more are present, that combination is defined as metabolic syndrome.
The five criteria are: a large waist circumference, elevated triglycerides, low HDL cholesterol, elevated blood pressure, and elevated fasting blood sugar. Three out of five qualifies. Many people have all five without being told they have a recognized clinical pattern.
The reason this cluster matters more than the individual parts is compounding. Each risk factor on its own raises cardiovascular risk modestly. But they reinforce each other biologically. The combination produces more inflammatory signaling, more arterial stress, and more metabolic dysfunction than any single factor would predict. Understanding what each criterion means, and what drives each one, is the starting point for addressing the whole picture.
What Are the Five Criteria and What Does Each One Mean?
Large waist circumference. The clinical thresholds are 40 inches or more in men and 35 inches or more in women. This criterion is a proxy for visceral adiposity, excess fat stored around the organs rather than under the skin. Visceral fat is not metabolically inert. It actively secretes pro-inflammatory cytokines and hormones that impair insulin signaling, raise blood pressure, and alter lipid metabolism. It is the central driver of the other four criteria in most people with metabolic syndrome. Waist circumference predicts cardiovascular risk better than BMI because it captures visceral fat distribution that BMI misses.
Elevated triglycerides. The threshold is 150 mg/dL or higher on a fasting blood test (or being on medication to manage triglycerides). Triglycerides are fat particles that circulate in the blood after meals. Chronically elevated fasting triglycerides reflect excess carbohydrate intake, insulin resistance, or both. The liver packages excess glucose and fructose into triglycerides and releases them as VLDL. Elevated VLDL competes with HDL in the circulation and contributes to the formation of small dense LDL particles, which are more atherogenic than large buoyant LDL. Triglycerides above 150, especially combined with low HDL, is one of the strongest clinical signals of insulin resistance. This is covered in more depth in the article on insulin resistance and heart disease.
Low HDL cholesterol. Below 40 mg/dL in men, below 50 mg/dL in women. HDL carries cholesterol away from arterial walls and back to the liver for disposal. It also carries anti-inflammatory proteins and helps maintain endothelial function. Low HDL is associated with accelerated plaque buildup and reduced arterial protection. In metabolic syndrome, HDL tends to be low because elevated triglycerides and insulin resistance promote the breakdown and clearance of HDL particles. You can read more about the complexity of HDL’s role in the article on HDL cholesterol and heart health.
Elevated blood pressure. The threshold for metabolic syndrome is 130/85 mmHg or higher (or being on blood pressure medication). At this level, the arterial wall is under sustained mechanical stress. Over time, elevated pressure damages the endothelium, promotes arterial stiffening, and triggers inflammatory responses in the vessel wall. In the context of metabolic syndrome, blood pressure tends to be elevated because insulin resistance causes sodium retention in the kidneys and activates the sympathetic nervous system. This is why blood pressure and insulin resistance are so frequently found together. The connections to arterial stiffness are direct.
Elevated fasting blood sugar. 100 mg/dL or higher (or being on diabetes medication). At 100 to 125, this is the prediabetes range. Above 126 is the diagnostic threshold for type 2 diabetes. But even within the officially normal range, research has found incremental cardiovascular risk. The article on why a normal fasting blood sugar can still carry cardiovascular risk goes into this in detail. For metabolic syndrome purposes, fasting glucose at or above 100 reflects significant enough insulin resistance that blood sugar regulation is beginning to slip.
Why Does the Combination Multiply Rather Than Just Add Risk?
This is the key insight that makes metabolic syndrome more than just a checklist. The five components are not independent risk factors that happen to co-occur. They share a common upstream driver, primarily insulin resistance and excess visceral fat, and they reinforce each other through overlapping biological mechanisms.
Visceral fat drives insulin resistance. Insulin resistance drives elevated triglycerides. Elevated triglycerides depress HDL. Insulin resistance also promotes sodium retention and sympathetic nervous system activation, raising blood pressure. And chronically elevated insulin with fluctuating blood sugar promotes endothelial dysfunction and inflammatory signaling throughout the arterial tree. This is the same inflammatory cascade described in the article on chronic low-grade inflammation and arterial damage.
The compounding effect shows up clearly in outcome data. A meta-analysis published in the Journal of the American College of Cardiology found that metabolic syndrome was associated with approximately a 2-fold higher risk of cardiovascular events and a 1.5-fold higher risk of all-cause mortality compared to people without it. Having all five criteria compounds the risk further. These are not additive numbers. The mechanisms interact.
The practical implication is that the interventions for all five criteria overlap heavily. You don’t need five separate treatment strategies. Reducing refined carbohydrate intake, increasing physical activity, reducing visceral fat, and improving sleep quality all move multiple criteria simultaneously. The same lifestyle changes that address one component tend to pull the others in the right direction.
This is also relevant to why cardiovascular risk can be high even when individual markers look borderline rather than clearly abnormal. Three markers that are each slightly elevated represent a different biological situation than one marker that is significantly elevated. The full cardiovascular risk factor framework addresses this: looking at the full picture rather than evaluating each number in isolation gives a more accurate assessment of where someone actually stands.

Frequently Asked Questions
How is metabolic syndrome diagnosed?
A healthcare provider checks five measurements: waist circumference, fasting triglycerides, HDL cholesterol, blood pressure, and fasting blood glucose. Three or more out of five meeting the threshold criteria (or being on medication that manages that criterion) qualifies as metabolic syndrome. There’s no single blood test for it. It requires pulling together measurements from a physical exam and a standard metabolic panel. Many doctors don’t explicitly use the term even when a patient meets the criteria.
Can metabolic syndrome be reversed?
Research consistently shows that the criteria for metabolic syndrome are highly responsive to lifestyle change. Studies on dietary modification, exercise programs, and weight loss interventions routinely show that participants who reduce visceral fat and improve insulin sensitivity see improvement across multiple criteria simultaneously. The term “reversal” is often used in research when a person no longer meets three or more criteria after intervention. How durable that reversal is depends on whether the lifestyle changes are maintained.
Is metabolic syndrome the same as prediabetes?
They overlap significantly but are not identical. Prediabetes is defined specifically by fasting glucose between 100 and 125 mg/dL or a hemoglobin A1c between 5.7% and 6.4%. Metabolic syndrome includes an elevated fasting glucose criterion but also requires several other components. Many people with prediabetes also meet the criteria for metabolic syndrome, and vice versa. The shared upstream driver is insulin resistance, which connects both conditions to the same metabolic and cardiovascular risk profile.
Should I worry if I only meet two of the five criteria?
Two criteria don’t qualify as metabolic syndrome by definition, but they’re worth taking seriously. Research on cardiovascular risk shows a graded relationship: more criteria present equals more risk, even below the formal threshold of three. Two borderline criteria combined with a family history of cardiovascular disease, smoking, or other risk factors represent a meaningful signal. The practical response is the same regardless of the label: addressing the upstream drivers through diet, activity, and sleep gives you leverage across all five criteria simultaneously.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
Get the Free Book →* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.