
Hemoglobin A1C and Heart Disease: What Your 3-Month Blood Sugar Average Reveals
Hemoglobin A1C and Heart Disease: What Your 3-Month Blood Sugar Average Reveals
Hemoglobin A1C is best known as a diabetes test. But cardiologists are paying close attention to A1C in people who aren’t diabetic — because even slightly elevated A1C, within the “normal” range, has been associated with incrementally higher cardiovascular risk in multiple large studies.
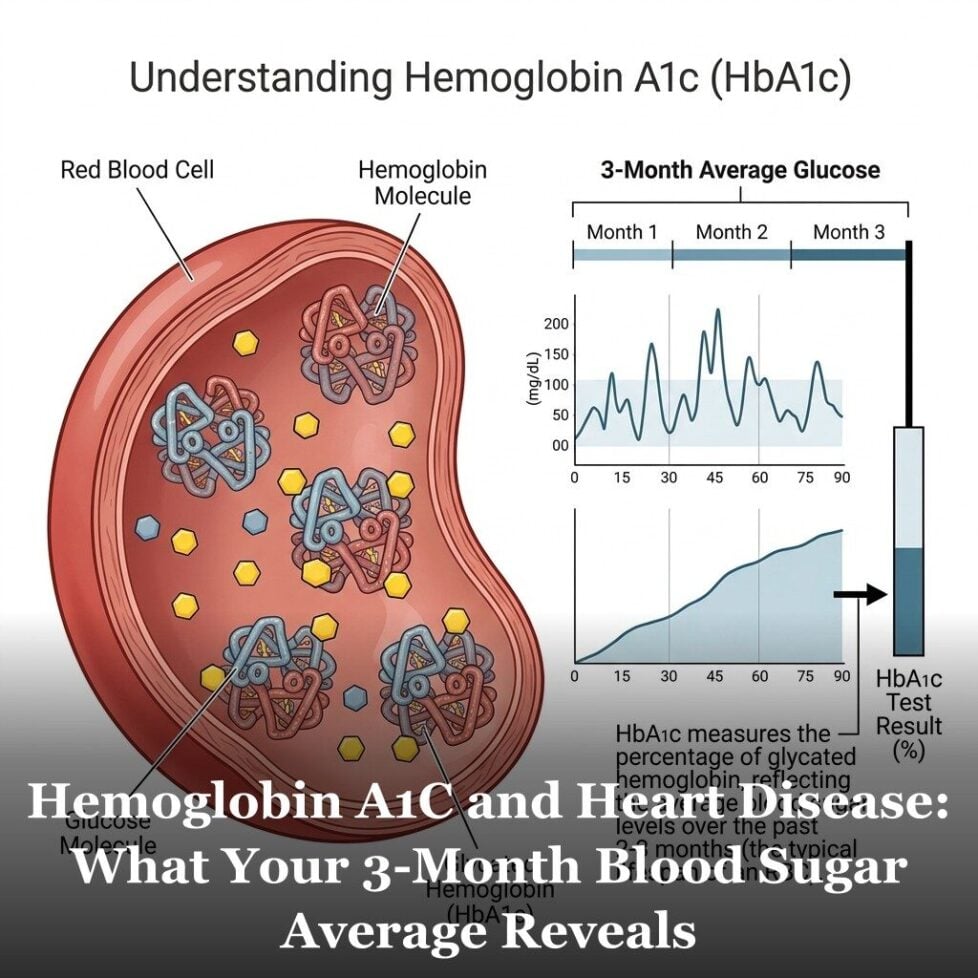
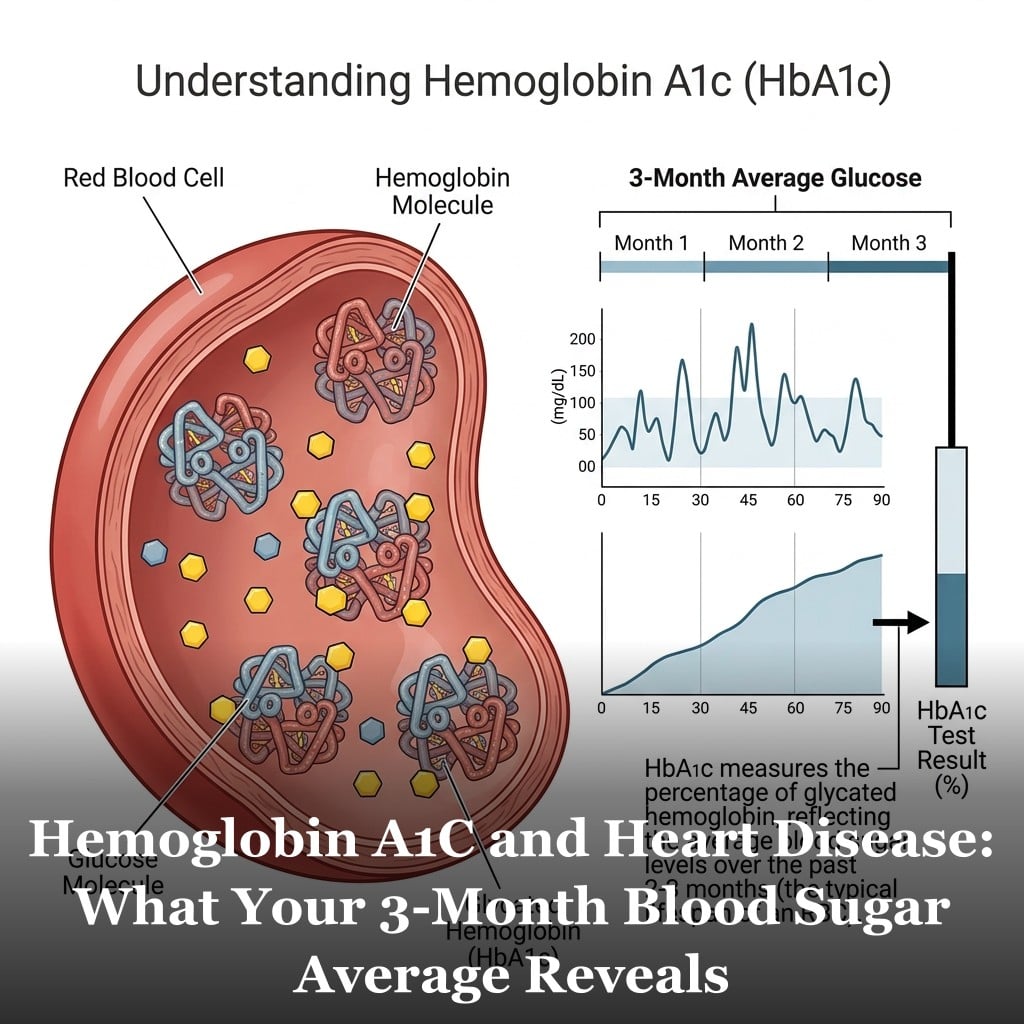
A1C reflects your average blood sugar over roughly three months. It measures what percentage of your hemoglobin has glucose attached to it. And the cardiovascular significance of this number starts before you cross into pre-diabetic territory.
What A1C Actually Measures
When blood glucose is elevated, some of it attaches to hemoglobin — the protein inside red blood cells that carries oxygen. This attachment, called glycation, is irreversible for the life of the red blood cell. Since red blood cells live about 90-120 days, A1C provides a running average of blood sugar exposure over roughly three months.
A standard fasting glucose test tells you where your blood sugar is at a single moment. A1C tells you where it’s been. That’s why A1C is so useful: it’s harder to game with a single day of careful eating before the test, and it captures the pattern of glucose exposure that matters for long-term tissue health.
Standard A1C interpretation: Below 5.7% is normal. 5.7-6.4% is pre-diabetic. 6.5% and above is the diagnostic threshold for diabetes. But the cardiovascular story starts well below these boundaries.
Why Elevated Blood Sugar Damages Arteries Over Time
Glucose molecules that attach to hemoglobin also attach to proteins throughout the body — including proteins in blood vessel walls. This process, called advanced glycation end-products (AGEs) formation, damages the structural proteins in arteries over time. Collagen and elastin in arterial walls become stiff and cross-linked as AGE accumulation increases.
Elevated glucose also promotes inflammation in endothelial cells — the cells lining blood vessel walls. Chronically elevated blood sugar impairs nitric oxide production in endothelial cells, which reduces their ability to maintain arterial flexibility and healthy blood flow. This endothelial dysfunction is an early step in the development of arterial damage.
Oxidative stress increases with elevated glucose. Excess glucose in cells generates reactive oxygen species that damage cellular components. The combination of inflammation, oxidative stress, and structural protein damage creates conditions that accelerate the cardiovascular changes associated with aging.
The critical point is that this damage begins accumulating well before blood sugar levels reach diabetic thresholds. The process is gradual and cumulative. An A1C that’s been at 5.8% for a decade represents meaningfully more cumulative glucose exposure than one that’s been at 5.2%.
What Tests Go Deeper Than Standard A1C
For people who want a more detailed picture of their glucose health, several options exist beyond the standard fasting glucose and A1C.
Fasting insulin. Insulin is elevated long before blood sugar rises. High fasting insulin — even with normal glucose and A1C — is a sign of insulin resistance in early stages. This test isn’t routinely ordered but is available and inexpensive.
HOMA-IR. A calculation using fasting glucose and fasting insulin together to estimate insulin resistance. More sensitive than glucose alone for catching early metabolic dysfunction.
Post-meal glucose testing. Checking glucose one to two hours after a meal reveals whether you’re having significant glucose spikes that your A1C and fasting tests wouldn’t detect. Consumer continuous glucose monitors (CGMs) have made this accessible without a prescription in many regions.
For the complete picture of how blood sugar fits into overall cardiovascular risk alongside cholesterol, blood pressure, and inflammation, see the 12 cardiovascular risk factors.

Frequently Asked Questions
What is an optimal A1C for cardiovascular health?
Most standard guidelines define normal as below 5.7%. Research suggests that lower within the normal range appears more favorable for cardiovascular outcomes. Many functional and preventive medicine practitioners target A1C below 5.4% as an optimal goal. The relationship appears to be a gradient — lower is generally better, within the context of not having hypoglycemia.
Can I lower my A1C through lifestyle alone?
Yes, especially if you’re in the normal to pre-diabetic range. The most effective strategies include reducing refined carbohydrates and added sugar, increasing physical activity (which improves insulin sensitivity), losing visceral fat, improving sleep quality, and managing chronic stress. Some people see meaningful A1C reductions within 3 months of sustained dietary and lifestyle changes.
Should my doctor test my A1C even if I’m not diabetic?
A1C is increasingly recommended as part of standard cardiovascular risk assessment, not just diabetes screening. The American Heart Association has recognized blood glucose control as a cardiovascular risk factor. If your doctor hasn’t been tracking A1C and you have other metabolic risk factors — elevated triglycerides, low HDL, high waist circumference — it’s a reasonable request.
Is A1C accurate for everyone?
A1C can be inaccurate in people with certain conditions that affect red blood cell turnover — including iron deficiency anemia, hemolytic anemia, sickle cell trait, and certain other hemoglobin variants. If you have any of these conditions, discuss with your doctor whether alternative measures of glycemic control are more appropriate for you.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
Get the Free Book →* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.