
Why Blood Pressure Spikes at Night and What That Signals About Your Heart
Why Blood Pressure Spikes at Night and What That Signals About Your Heart
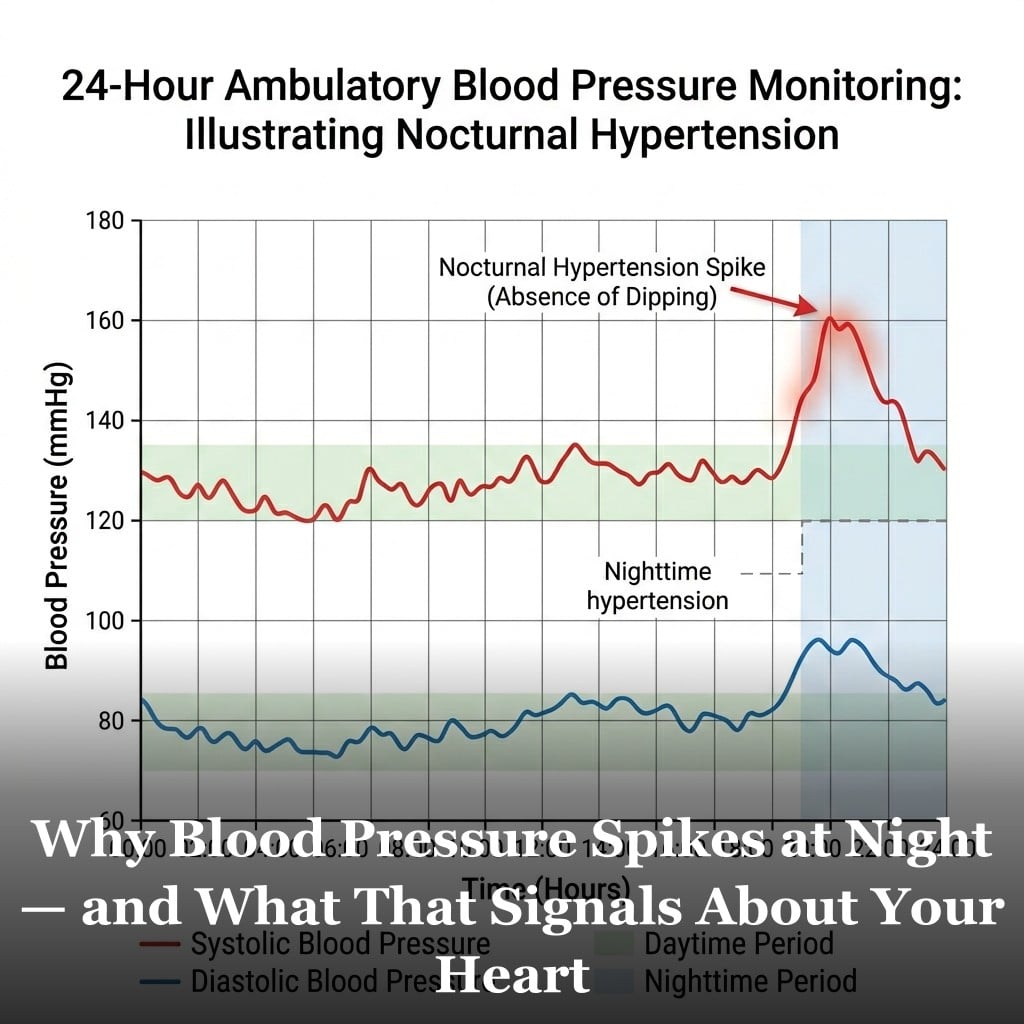
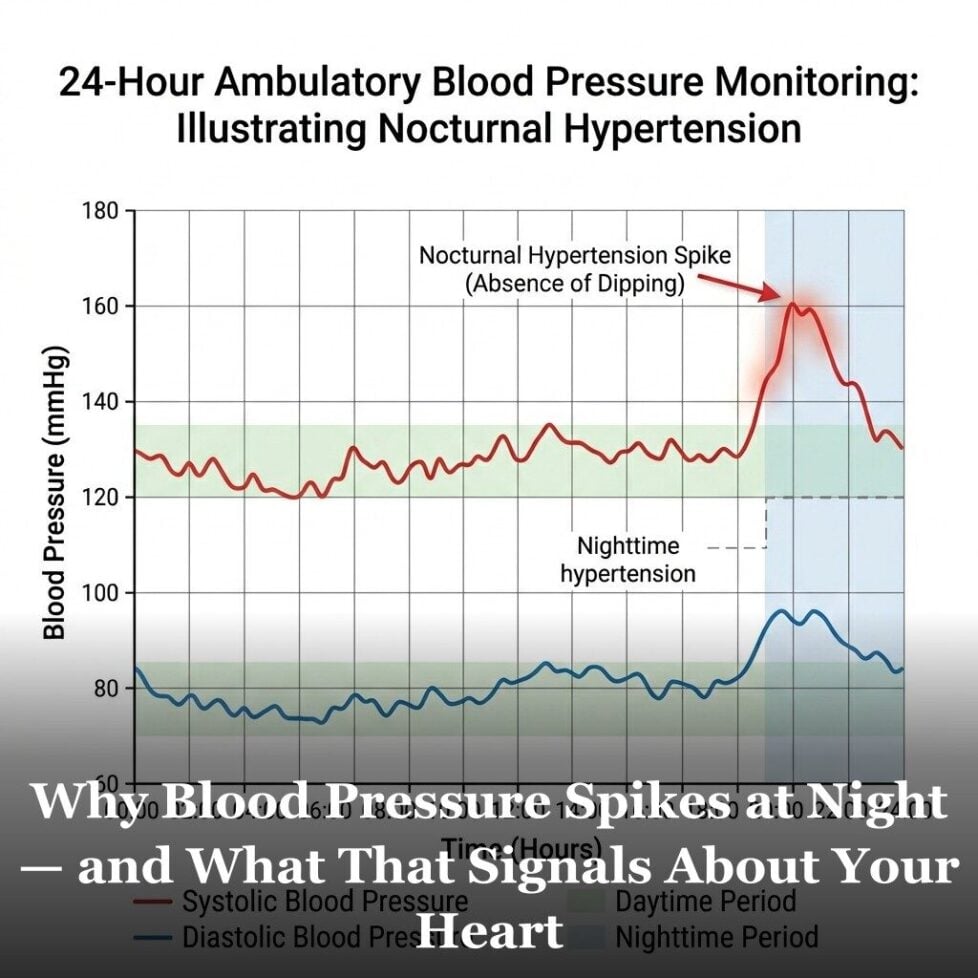
Blood pressure is supposed to drop while you sleep. This natural nighttime dip is a normal part of the cardiovascular system’s recovery cycle. But in a significant number of people, blood pressure doesn’t drop the way it should — or it rises during sleep. And this pattern is associated with greater cardiovascular risk than elevated daytime readings alone.
The problem is that your doctor’s office reading only captures a moment in time, typically during the day. What happens to your blood pressure when you’re asleep is invisible on a standard measurement. And for some people, the nighttime picture is the more clinically important one.
Why Blood Pressure Normally Drops During Sleep
The cardiovascular system is regulated in part by the autonomic nervous system, which has two main branches. The sympathetic branch activates the “fight or flight” response — raising heart rate, blood pressure, and alertness. The parasympathetic branch promotes the “rest and digest” state, slowing the heart and reducing blood pressure.
During normal, healthy sleep, parasympathetic activity increases and sympathetic tone decreases. Blood pressure typically dips 10-20% below daytime levels. This nocturnal dip is important for several reasons. It gives the heart a period of reduced workload. It allows blood vessels some relief from the pressures they’re under throughout the waking day. And it’s associated with lower overall cardiovascular risk.
People whose blood pressure dips normally during sleep are called “dippers” in cardiology research. Those whose blood pressure doesn’t dip — or dips less than 10% — are called “non-dippers.” Those whose pressure actually rises at night are called “reverse dippers” or “risers.”
What Causes Non-Dipping and Reverse Dipping
Several conditions are associated with blunted or absent nighttime blood pressure dipping. Understanding them helps explain why this pattern matters and who is most at risk.
Sleep apnea is one of the most common causes. When breathing repeatedly stops during sleep, the body activates sympathetic stress responses — raising heart rate and blood pressure with each episode. People with untreated obstructive sleep apnea frequently show non-dipping or reverse-dipping patterns. Treatment of sleep apnea often normalizes the nighttime blood pressure pattern.
Chronic kidney disease is strongly associated with non-dipping. The kidneys play a central role in blood pressure regulation, and impaired kidney function disrupts the normal nocturnal patterns.
Autonomic dysfunction — including diabetic autonomic neuropathy and certain neurological conditions — can impair the normal parasympathetic surge during sleep.
Excessive sodium intake combined with salt sensitivity can produce non-dipping patterns by disrupting the fluid balance mechanisms that normally allow nocturnal pressure reduction.
Advanced age is associated with a gradual loss of normal dipping patterns, partly because autonomic regulation becomes less robust with age.
What This Means for Your Cardiovascular Health
Standard office blood pressure readings don’t capture the nighttime picture at all. A person whose daytime readings look well-controlled but who is a reverse-dipper with elevated nighttime pressure is at meaningfully higher cardiovascular risk than their office readings suggest.
If you have conditions associated with non-dipping — especially sleep apnea, kidney disease, or diabetes — it’s worth asking your doctor whether ambulatory monitoring would give a more complete picture of your blood pressure control.
Sleep quality and sleep architecture play a meaningful role in cardiovascular health beyond just blood pressure. Poor sleep is independently associated with elevated cardiovascular risk through multiple mechanisms, which we’ll explore in more detail later in this series.
For the complete picture of blood pressure risk factors and how they interact with other cardiovascular markers, see the 12 cardiovascular risk factors. And for how arterial changes underlie many blood pressure patterns, the arterial stiffness article provides useful context.

Frequently Asked Questions
How would I know if I have non-dipping blood pressure?
You can’t know from standard office readings. The only way to detect nocturnal patterns is ambulatory blood pressure monitoring — a device worn for 24 hours that takes regular readings throughout the day and night. If you have sleep apnea, diabetes, chronic kidney disease, or resistant hypertension, ask your doctor whether ABPM would be appropriate for a more complete assessment.
Can treating sleep apnea improve blood pressure?
In many cases, yes. Effective treatment of obstructive sleep apnea — typically with CPAP therapy — has been shown to improve nocturnal blood pressure patterns and, in some studies, to modestly reduce daytime blood pressure as well. People with both sleep apnea and hypertension often show meaningful improvements in blood pressure control after effective sleep apnea treatment.
Is it bad if blood pressure dips too much at night?
Excessive nocturnal dipping — typically defined as more than 20% below daytime levels — is also a clinical concern in some contexts. Extreme dippers may have inadequate perfusion of certain organs during deep sleep. However, extreme dipping is much less common than non-dipping as a clinical problem, and modest dipping (10-20%) is the healthy pattern most cardiologists aim for.
Does caffeine affect nighttime blood pressure?
Caffeine raises blood pressure acutely for several hours after consumption. People who consume caffeine in the afternoon or evening may have elevated blood pressure at the time they would normally be entering the nocturnal dip phase. For people who are sensitive to caffeine’s cardiovascular effects, avoiding caffeine after early afternoon is a reasonable precaution for supporting normal nocturnal blood pressure patterns.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
![]()
![]()
![]()
![]()
![]()
![]()
![]()