
Why Your LDL Number Can Be Normal and Your Heart Risk Still High
Why Your LDL Number Can Be Normal and Your Heart Risk Still High
Your doctor checked your cholesterol. LDL came back at 110 mg/dL. That’s in the normal range, so you got the all-clear. But there’s a dimension of LDL that the standard test doesn’t capture. It’s getting more attention from cardiologists who want a fuller picture of cardiovascular risk.
Standard LDL tests measure how much cholesterol your LDL particles are carrying. What they don’t measure is how many particles there are, or how small and dense those particles are. Those two details can change the risk picture significantly.
Two people with identical LDL cholesterol readings can have very different particle counts. And researchers have found that particle characteristics may be a stronger predictor of cardiovascular risk than LDL-C alone in certain patient populations.
What Does a Standard LDL Test Actually Measure?
The number your doctor reports as “LDL” is technically LDL-C: LDL cholesterol. It measures the total amount of cholesterol being carried inside LDL particles, calculated indirectly from your total cholesterol, HDL, and triglycerides.
What it doesn’t measure is the number of individual LDL particles circulating in your bloodstream. A person could have a low LDL-C but carry a high number of small, dense particles. That situation can look fine on a standard panel while telling a different story on advanced testing.
This limitation has been known in cardiology research for decades. Standard LDL-C remains widely used because it’s inexpensive and useful for most people. But for those with metabolic risk factors, the standard test may not tell the whole story.
Why Particle Size and Density Matter
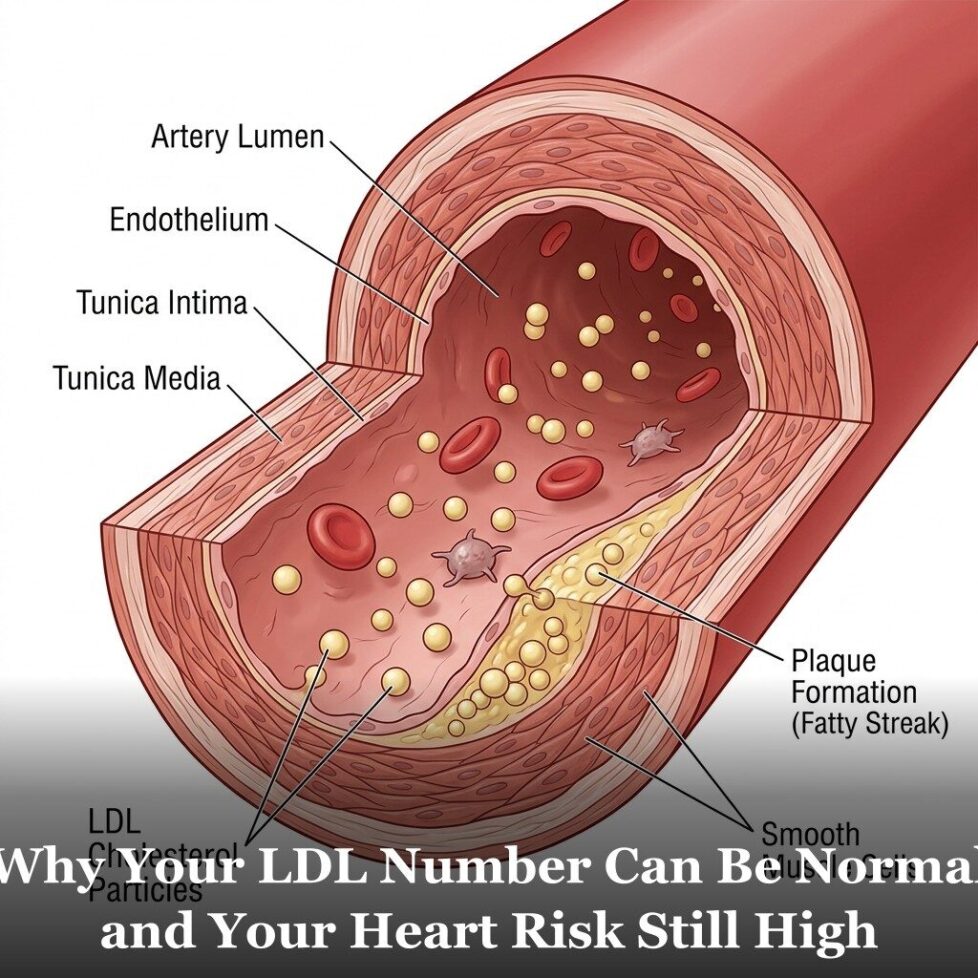
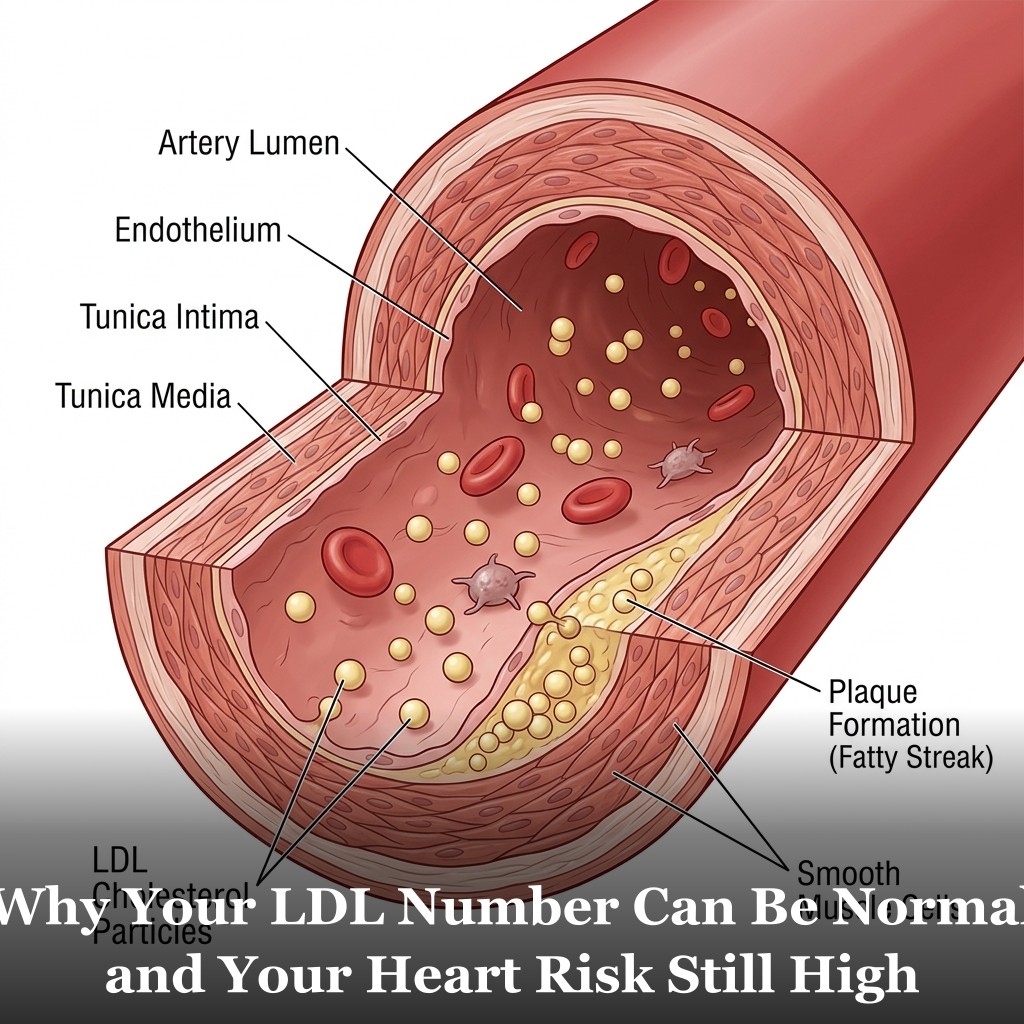
LDL particles aren’t all the same size. Some are large and buoyant. Others are small and dense. The difference matters because small, dense LDL particles behave differently in the body.
Small, dense particles are more easily oxidized. Oxidized LDL is more likely to embed in artery walls and contribute to the buildup associated with cardiovascular disease. Large, buoyant LDL particles appear to be less prone to this process, according to the available research.
The proportion of small, dense particles tends to increase when triglycerides are elevated and HDL is low. This combination is frequently associated with insulin resistance. It helps explain why two people with the same LDL-C can have different cardiovascular risk profiles.
If you want to understand the full picture of how these factors interact, the 12 cardiovascular risk factors article covers each one and how they connect.
Tests That Give You a Fuller Picture
Several tests measure what standard LDL-C doesn’t. They aren’t routinely ordered but are available if your doctor thinks advanced testing is appropriate for you.
LDL particle number (LDL-P). This test uses NMR spectroscopy to directly count the number of LDL particles in your blood. It gives both total particle count and size distribution. Multiple large studies have found LDL-P to be a stronger predictor of cardiovascular risk than LDL-C.
ApoB. Every LDL particle carries exactly one ApoB protein on its surface. So measuring ApoB gives you a direct count of LDL particles. ApoB is simpler and less expensive than full particle counting. Many cardiologists now consider it a better routine risk marker than standard LDL-C. We cover this in depth in the ApoB article.
sdLDL. Small, dense LDL can be measured directly. This test is less widely available than ApoB but is an option through specialty labs.
These tests aren’t necessary for everyone. If your metabolic markers are all healthy, standard LDL-C is probably telling you most of what you need to know. But if you have elevated triglycerides, low HDL, borderline glucose, or a family history of early heart disease, advanced lipid testing is worth a conversation with your doctor.

Frequently Asked Questions
My LDL is normal. Do I need to worry about particle size?
For most people with healthy metabolic markers across the board, standard LDL-C is usually enough. Advanced testing tends to be most useful when other risk factors are present — elevated triglycerides, low HDL, borderline glucose, or a strong family history of early heart disease. If any of those apply, it’s worth asking your doctor about ApoB or LDL particle testing.
Is an ApoB or LDL-P test expensive?
ApoB is a relatively inexpensive blood test and is increasingly covered by insurance when there’s a clinical reason for it. LDL particle number testing (NMR) is more specialized and may involve out-of-pocket costs depending on your coverage. Your doctor or a cardiologist can advise on what’s appropriate for your situation.
What causes a higher proportion of small, dense LDL particles?
The proportion of small, dense LDL tends to increase when triglycerides are elevated, HDL is low, and in people with insulin resistance. High refined carbohydrate intake and low physical activity are associated with this pattern. Genetics also plays a role for some people.
Can diet and exercise change my LDL particle profile?
Research suggests that reducing refined carbohydrates, increasing physical activity, and improving overall metabolic health can shift LDL particles toward the larger, less dense pattern. Strategies that lower triglycerides and raise HDL tend to have a favorable effect on particle characteristics. Speak with your doctor about what’s appropriate for your situation.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
Get the Free Book →* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.