
Diastolic vs. Systolic Blood Pressure: Which Number Should You Really Be Watching?
Diastolic vs. Systolic Blood Pressure: Which Number Should You Really Be Watching?
When your doctor reads out your blood pressure, they usually focus on the top number. “Your systolic is 138” — and that’s what sticks in your mind. But the bottom number, diastolic, tells a different part of the story. And the relationship between the two numbers shifts significantly as people age.
Understanding what each number actually measures helps you have a more informed conversation with your doctor and get more out of your blood pressure readings. It also changes which number you should be watching most closely at different stages of life.
What Each Number Measures
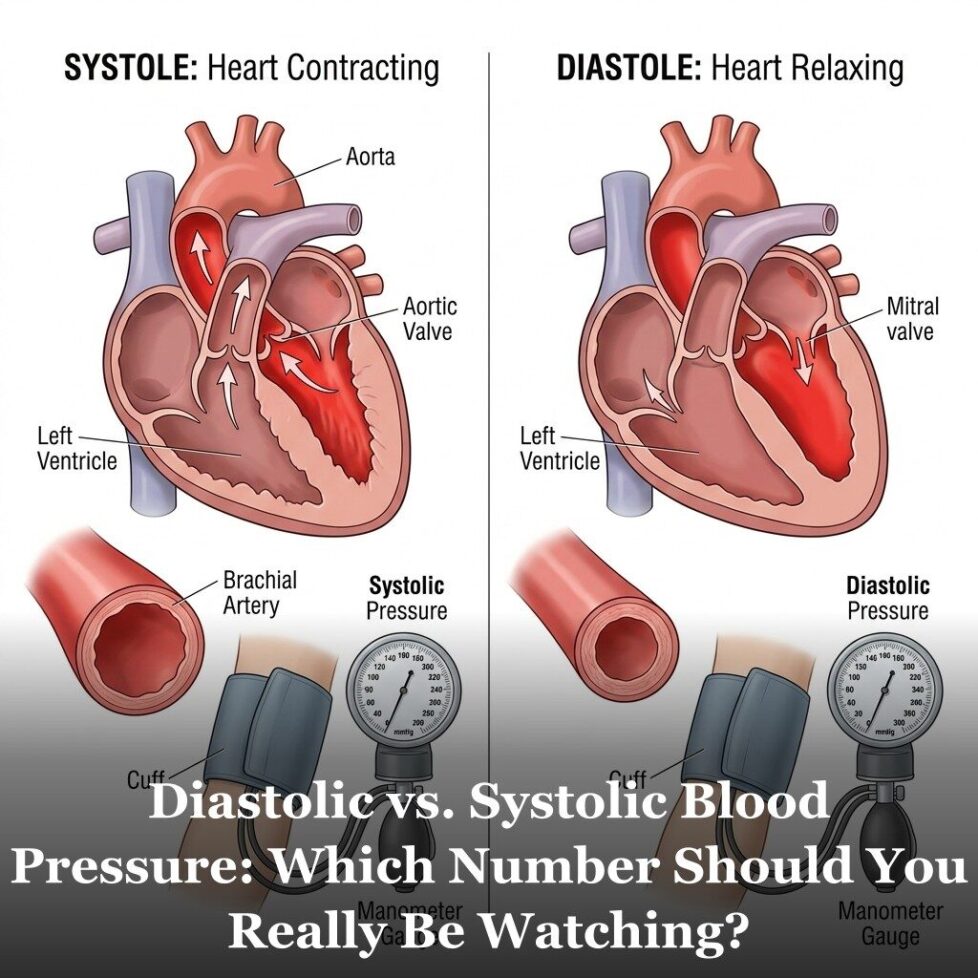
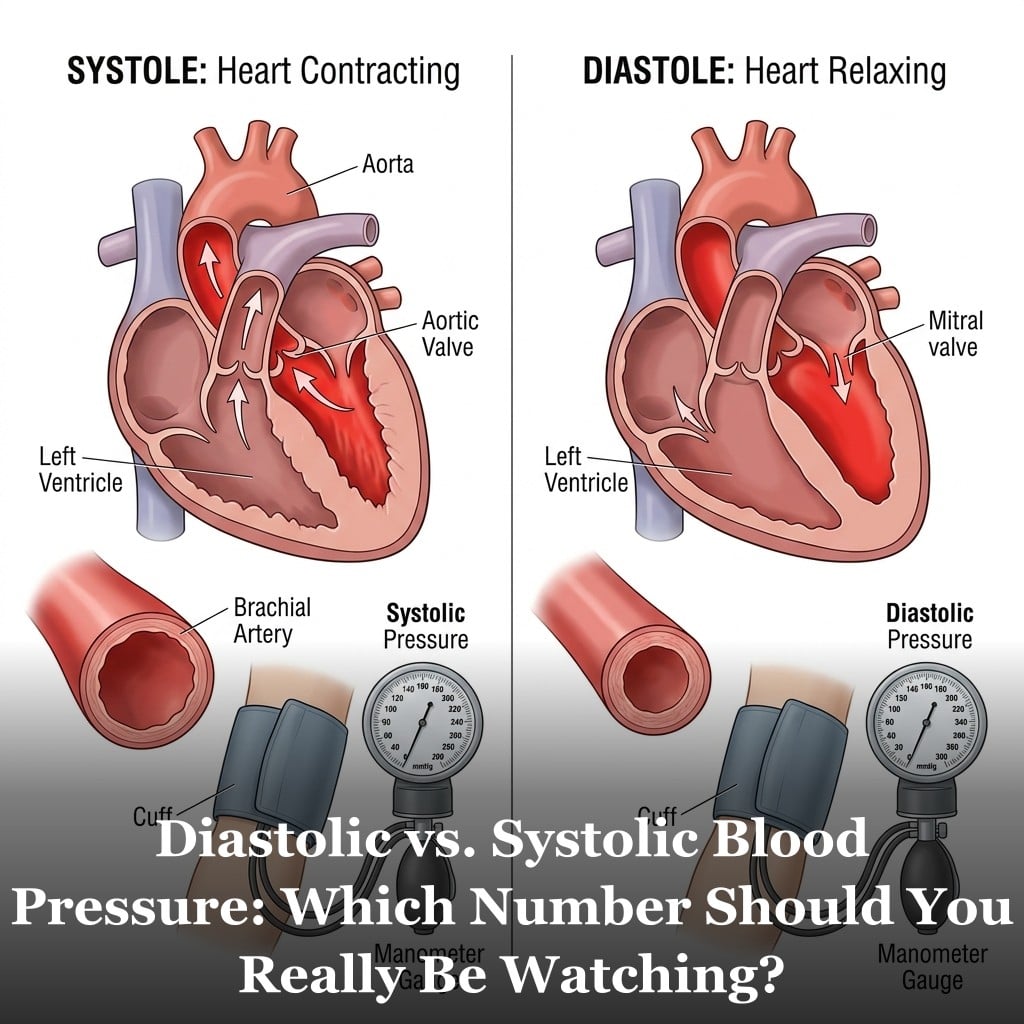
Systolic blood pressure is the pressure in your arteries at the moment your heart contracts and pushes blood out. It’s the peak pressure in the system. Diastolic is the pressure in your arteries when your heart is relaxed between beats, refilling before the next contraction. It’s the baseline pressure that your arterial walls are under continuously.
A reading of 120/80 means: systolic pressure of 120 mmHg at the moment of contraction, diastolic pressure of 80 mmHg between beats. The slash between the numbers represents the heartbeat itself.
Both numbers are clinically important, but they reflect different aspects of cardiovascular function. Systolic pressure reflects the force generated by the heart and the stiffness of the arteries it’s pushing against. Diastolic pressure reflects the resistance in the smaller arterial vessels and the resting tone of the vascular system.
When Diastolic Matters Most and When Systolic Takes Over
In younger adults (under about 50), diastolic hypertension is the more common concern. Elevated diastolic pressure reflects increased resistance in the smaller peripheral blood vessels — a pattern associated with early-stage hypertension in younger populations. The arteries are still relatively elastic, so systolic stays manageable while diastolic climbs.
In adults over 50, the pattern tends to reverse. As major arteries stiffen with age, systolic pressure rises while diastolic often stays flat or even falls. Isolated systolic hypertension — where only the top number is elevated — becomes the most common form of hypertension in older adults.
This age-related shift has important clinical implications. Older adults with high systolic but normal diastolic aren’t experiencing the same cardiovascular process as younger adults with high diastolic. The treatment approach and underlying mechanisms differ.
Multiple large studies, including analyses from the Framingham Heart Study, have found that after age 60, systolic blood pressure becomes a stronger predictor of cardiovascular risk than diastolic pressure. In older adults, controlling systolic pressure has been shown to meaningfully reduce cardiovascular events in clinical trials.
What to Watch for at Your Next Blood Pressure Reading
A few practical points for interpreting your own readings:
Don’t ignore either number. Both matter, just in different ways. Elevated systolic in an older adult and elevated diastolic in a younger adult are both worth addressing, even if they reflect different underlying processes.
Look at the pattern over time. A single reading gives limited information. Your doctor should be tracking trends across multiple visits under comparable conditions. Home blood pressure monitoring can provide much more data than occasional office visits.
Calculate your pulse pressure. As we covered in the pulse pressure article, the gap between your two numbers adds another dimension to the picture. A widening pulse pressure over time can be clinically significant even when individual numbers are borderline.
Understand white coat hypertension. Many people show elevated readings at the doctor’s office due to the stress of the visit. Home monitoring or ambulatory monitoring (wearing a blood pressure cuff throughout the day) gives a more representative picture. If your office readings are consistently elevated but you feel fine, ask your doctor about ambulatory monitoring.
For the broader context of where blood pressure fits in the full cardiovascular risk picture, see the 12 cardiovascular risk factors.

Frequently Asked Questions
Which number is more dangerous to have elevated?
It depends on your age. In adults under 50, elevated diastolic tends to be the more common concern and reflects peripheral vascular resistance. In adults over 50, systolic hypertension becomes the more prevalent and clinically significant pattern. Both matter, and both are addressed in treatment guidelines. Your doctor interprets your readings in the context of your age, overall risk, and other health factors.
Is a diastolic of 90 dangerous?
A diastolic of 90 places you in Stage 1 hypertension territory according to most guidelines (the threshold is 80 for Stage 1 and 90 for Stage 2). This level warrants a conversation with your doctor about lifestyle modifications and whether medication is appropriate based on your overall cardiovascular risk profile. A single reading of 90 is less meaningful than a sustained pattern across multiple readings.
Why does blood pressure vary throughout the day?
Blood pressure follows a circadian rhythm. It’s typically lowest during sleep, rises sharply in the morning (the ‘morning surge’), peaks in mid-afternoon, and gradually decreases through the evening. Emotional stress, physical activity, caffeine, a full bladder, and even the position you’re sitting in can all affect readings. This is why standardized conditions — sitting quietly for 5 minutes before measuring — matter for getting accurate readings.
Can you have high systolic but normal diastolic?
Yes. This is called isolated systolic hypertension, and it’s the most common form of hypertension in adults over 60. It reflects primarily age-related stiffening of the major arteries. Even with a diastolic in the 70s, a systolic consistently above 140 is associated with elevated cardiovascular risk and is addressed in hypertension treatment guidelines.
Get Your Free Heart Book
Your Doctor Checks Blood Pressure & Cholesterol: What About the Other 10?
Most heart attacks happen to people whose last checkup came back “fine.” This book covers the 12 risk factors your doctor may not be testing — in plain English, backed by research.
Get the Free Book →* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.