
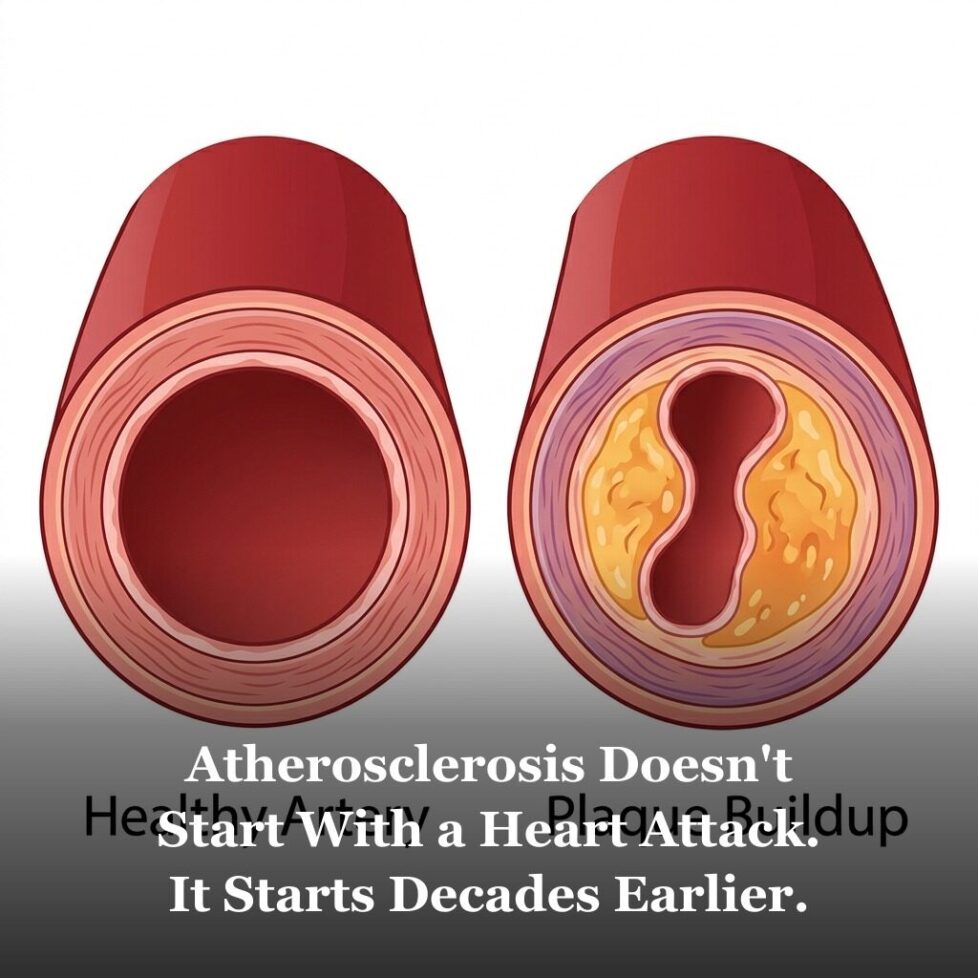
Atherosclerosis Doesn’t Start With a Heart Attack. It Starts Decades Earlier.
Atherosclerosis Doesn’t Start With a Heart Attack. It Starts Decades Earlier.
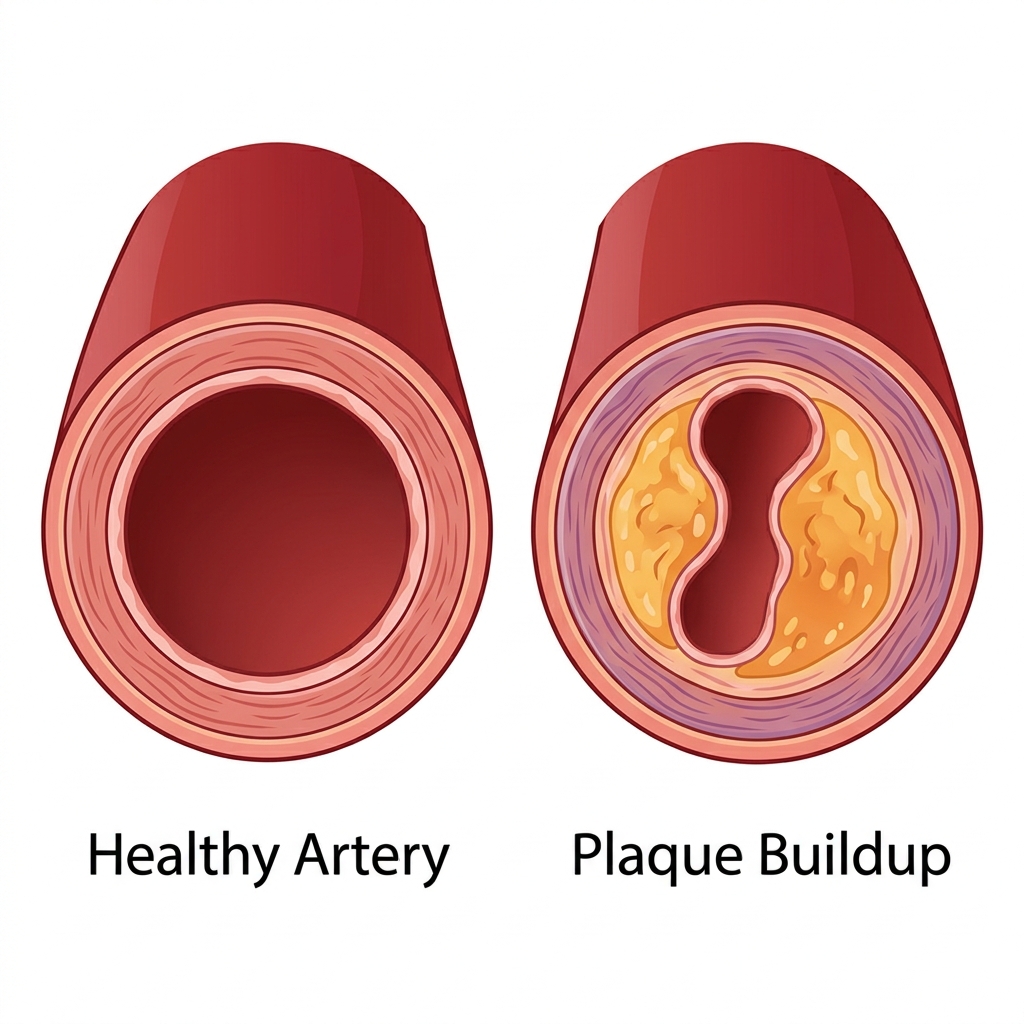
Atherosclerosis is the buildup of plaque inside arterial walls. It’s not a pipe-clogging process — it’s an inflammatory disease that often starts in your 20s and develops silently for decades. By the time symptoms appear, the disease has usually been progressing for 20 to 40 years.
The word atherosclerosis comes from the Greek words for gruel (athere) and hardening (sclerosis). Both parts of that name describe something real, but together they create a misleading picture of what actually happens inside an artery.
Most people imagine the process the way you’d imagine a pipe getting clogged: plaque builds up on the inside surface, the opening gets narrower, and eventually flow stops. That’s not quite right. Atherosclerosis begins inside the arterial wall itself, driven by inflammation, and it progresses through stages that have nothing to do with a pipe filling up from the inside.
Understanding the actual process matters because it changes what risk factors you pay attention to, what tests are worth asking for, and why someone can have a heart attack without ever being told they had “bad arteries.”

What Atherosclerosis Actually Is: An Inflammatory Disease, Not a Plumbing Problem
The process starts with the endothelium. That’s the single-cell-thick lining of every artery, about the width of a human hair, that separates the blood from the arterial wall beneath it. A healthy endothelium is smooth, actively anti-inflammatory, and prevents anything from the bloodstream from getting into the wall itself.
When the endothelium is damaged or inflamed, it becomes permeable. LDL particles, which are small enough to pass through, begin to enter the arterial wall. Once inside, they get oxidized by free radicals in the tissue. Oxidized LDL is chemically different from native LDL, and the immune system treats it as a threat.
Immune cells called monocytes are recruited from the bloodstream. They enter the arterial wall and transform into macrophages. Those macrophages try to eat the oxidized LDL, but when they consume enough of it, they become engorged. Researchers call these engorged cells foam cells. A collection of foam cells is called a fatty streak, and it’s the earliest visible stage of atherosclerosis.
The fatty streak doesn’t cause symptoms. It doesn’t narrow the artery meaningfully. But the inflammatory process that created it is ongoing, and over time, the lesion grows.
How Plaque Develops: From Fatty Streak to Fibrous Cap
As foam cells die, they release their lipid contents into the arterial wall, creating a growing lipid pool. The body’s repair response surrounds this pool with smooth muscle cells and a connective tissue cap, called the fibrous cap. This is what’s typically referred to as an atherosclerotic plaque.
A mature plaque has two main components: the soft, lipid-rich necrotic core in the center, and the fibrous cap covering it. The cap keeps the contents of the plaque away from the bloodstream. As long as the cap is intact and thick, the plaque is considered stable.
But the same inflammatory environment that created the plaque also weakens the cap over time. Matrix metalloproteinases (enzymes produced by inflammatory cells) degrade the collagen that gives the cap its strength. Where the cap is thinnest, it becomes vulnerable to rupture.
When a vulnerable plaque ruptures, the lipid-rich contents of the core come into contact with the bloodstream. Platelets rush to the site, sensing the exposed material as if it were a wound. A clot forms. If that clot is large enough to block the artery, it’s a heart attack. If it breaks off and travels to a smaller vessel, it can cause a stroke. For more on that clotting process, see the article on platelet activity and blood clots.
Why “How Much” Plaque Isn’t the Only Thing That Matters
This is one of the most important and counterintuitive things about atherosclerosis: the size of a plaque and its danger level are not the same thing.
Stable plaques can be large and cause significant narrowing without being immediately dangerous. Vulnerable plaques can be relatively small, barely narrowing the artery at all on an angiogram, and still rupture suddenly and cause a massive cardiac event.
This is why coronary angiography (the dye-injection imaging often used to assess blockages) can miss dangerous lesions. It shows the lumen of the artery, not the plaque inside the wall. A small vulnerable plaque may look unremarkable on an angiogram right up until it ruptures.
Research has associated several factors with plaque vulnerability: a large lipid core, a high ratio of inflammatory cells to smooth muscle cells, thin fibrous cap, high levels of oxidized LDL, and active neovascularization (new blood vessel growth inside the plaque itself, which can create additional entry points for rupture).
What Accelerates Atherosclerosis
Multiple factors have been consistently associated in research with accelerating the atherosclerotic process. Most work through one of three mechanisms: damaging the endothelium, increasing LDL oxidation, or amplifying inflammation.
Oxidized LDL. Regular LDL is not the direct problem — oxidized LDL is. Factors that increase LDL oxidation include smoking, low antioxidant intake, high blood sugar, and high levels of small dense LDL particles (which are more susceptible to oxidation than large LDL particles).
High blood pressure. Mechanical stress from elevated blood pressure damages the endothelium, particularly at arterial branch points where flow is turbulent. This is why atherosclerosis tends to develop most heavily at bends and bifurcations in the coronary and carotid arteries.
Elevated homocysteine. Homocysteine is an amino acid that damages the endothelial lining directly when chronically elevated. Research has associated high homocysteine with both accelerated plaque formation and increased plaque vulnerability.
Insulin resistance and high blood sugar. Glucose promotes the glycation of LDL particles, making them more prone to oxidation. Insulin resistance also raises triglycerides and lowers HDL, creating a lipid profile more associated with atherogenesis.
Low nitric oxide production. Nitric oxide is the endothelium’s primary anti-atherogenic signal. It keeps the endothelium smooth, prevents LDL from entering the wall, and maintains arterial flexibility. When nitric oxide production is impaired, the endothelium is more vulnerable to the initial steps of atherosclerosis.
Smoking. Smoking damages the endothelium directly, increases oxidative stress, raises fibrinogen, lowers HDL, and promotes inflammation. It’s one of the most potent accelerators of atherosclerosis known.

What Research Associates With Slowing Atherosclerosis
The same mechanisms that accelerate the disease point to what can slow it.
Antioxidants. Since LDL oxidation is central to plaque formation, antioxidants that reduce oxidative stress in the arterial wall are a natural area of research focus. Vitamin C, vitamin E, polyphenols from fruits and vegetables, and CoQ10 have all been studied in this context. The research on isolated antioxidant supplementation is mixed, but dietary patterns high in antioxidants (Mediterranean diet, for example) have more consistent associations with reduced atherosclerotic progression.
Omega-3 fatty acids. EPA and DHA have been associated with anti-inflammatory effects in the arterial wall, reduced triglycerides, and in some studies, reduced plaque progression. They also support healthier platelet function, which matters at the vulnerable plaque stage.
Blood pressure management. Reducing mechanical stress on the endothelium, through medication, diet, exercise, or stress management, slows the rate of endothelial injury at the sites where atherosclerosis tends to develop.
Not smoking. The benefit of smoking cessation on cardiovascular risk is measurable within years. The endothelium begins recovering relatively quickly once the constant chemical exposure stops.
Regular exercise. Physical activity has been associated with improved endothelial function, higher nitric oxide production, reduced inflammation, and more favorable lipid patterns. Even moderate aerobic exercise shows consistent associations with slower atherosclerotic progression in imaging studies.
Coronary Calcium Scoring: A Window Into Your Arterial Health
One of the most useful tests for assessing atherosclerotic burden is the coronary artery calcium (CAC) score. It’s a low-dose CT scan that measures calcified plaque in the coronary arteries. Calcification is a later stage of plaque development, but its presence is a reliable marker that atherosclerosis has been active.
A score of zero indicates no detectable calcified plaque, and research has associated a zero score with very low near-term cardiovascular event risk, even in people with elevated LDL. A score above 100 meaningfully raises estimated risk. A score above 400 places someone in the high-risk category.
The test is inexpensive (often $100-150 without insurance), takes about 10 minutes, and doesn’t require contrast dye or fasting. Major cardiology guidelines, including from the American College of Cardiology, now recommend it for intermediate-risk patients where the result can change treatment decisions.
It’s worth asking your doctor about, particularly if you have risk factors but a standard lipid panel that looks relatively normal.
The Full Picture: Atherosclerosis and the 12 Cardiovascular Risk Factors
Atherosclerosis doesn’t develop from a single cause. It’s the endpoint of a process driven by multiple overlapping risk factors — most of which are measurable and many of which are modifiable.
The 12 cardiovascular risk factors that research has consistently identified represent the upstream inputs that drive atherosclerotic progression. Oxidized LDL, inflammation, blood pressure, blood sugar, homocysteine, nitric oxide deficiency, and several others all feed into the disease at different stages. Understanding them individually and how they interact gives you a far more useful picture than any single number from a standard checkup.
For a deeper look at specific factors, the articles on small dense LDL cholesterol, homocysteine, and nitric oxide are directly relevant to how atherosclerosis develops and what can be done to slow it.

*These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
Frequently Asked Questions
Is atherosclerosis the same thing as “hardening of the arteries”?
They overlap but aren’t identical. “Hardening of the arteries” typically refers to arteriosclerosis, a general loss of arterial elasticity that happens with aging. Atherosclerosis is a specific subtype involving inflammatory plaque buildup inside the arterial wall. Both contribute to increased arterial stiffness, but atherosclerosis carries the additional risk of plaque rupture. Many older adults have both occurring simultaneously, which is why the terms are often used interchangeably even though they describe different processes.
Can atherosclerosis be reversed — or is it a one-way process?
The research suggests that early-stage atherosclerosis can be slowed and that some regression of established plaque is possible with aggressive intervention. Statin therapy in particular has been shown in intravascular ultrasound studies to produce modest but measurable plaque regression. The REVERSAL trial documented that intensive lipid lowering produced actual plaque regression compared to modest treatment. Full reversal of advanced plaque is unlikely, but slowing or halting progression is a realistic and well-documented goal.
What’s the coronary calcium score test, and should you ask for one?
The coronary artery calcium (CAC) score is a low-dose CT scan that measures calcified plaque in the coronary arteries. It’s non-invasive, takes about 10 minutes, and doesn’t require contrast dye. A score of zero is associated with very low near-term cardiac event risk. Scores above 100 or 400 indicate progressively higher risk. Major cardiology guidelines now recommend it for intermediate-risk patients where it can meaningfully change treatment decisions. If you have risk factors but borderline cholesterol numbers, it’s worth asking your doctor about.
Why does a “normal” cholesterol level not guarantee your arteries are healthy?
Standard cholesterol panels measure total LDL, HDL, and triglycerides — but they don’t measure LDL particle size, oxidized LDL, or other drivers of plaque formation. Research has shown that small dense LDL particles are more atherogenic than large particles at the same total LDL level. Homocysteine, C-reactive protein (inflammation), lipoprotein(a), and blood sugar also contribute to atherosclerosis independently of standard cholesterol. A person can have a normal lipid panel and still have significant underlying arterial disease.
What’s the difference between a stable plaque and a dangerous one?
A stable plaque has a thick fibrous cap and a smaller lipid core. It may narrow the artery noticeably but is less likely to rupture suddenly. A vulnerable plaque has a thin cap and a large, soft, lipid-rich core with high levels of inflammatory cells. It may cause less visible narrowing than a stable plaque — and may look relatively minor on an angiogram — but is far more likely to rupture, triggering the sudden clot formation that causes most heart attacks. This is why “how blocked” an artery looks isn’t the whole story.
Start Earlier. The Disease Does.
The most important takeaway from the research on atherosclerosis is the timeline. By the time a person is in their 40s or 50s and learns they have “some plaque,” the process has typically been running for two or three decades. The fatty streaks that preceded it were there in their 20s.
That’s not meant to be alarming. It’s meant to reframe when the relevant decisions happen. The choices that matter most for arterial health are the ones made in the decades before a problem becomes visible on any test. The upstream risk factors — the ones that create oxidative stress, damage the endothelium, and drive inflammation — are where the real leverage is.
Understanding atherosclerosis in full means understanding the 12 cardiovascular risk factors that drive it, including the ones that rarely come up in a standard checkup. The articles on small dense LDL cholesterol and homocysteine are a good place to continue.
Get the Free Heart Health Guide
A plain-English overview of the 12 cardiovascular risk factors — what they are, how they connect, and what to ask your doctor.
Download Free Guide →*These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. This article is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider before making changes to your health regimen.
References
- Enos WF, et al. Coronary disease among United States soldiers killed in action in Korea. JAMA. 1953;152(12):1090-1093. PMID: 13052433
- Libby P, et al. Atherosclerosis. Nature. 2011;473(7347):317-325. PMID: 21593864
- Stary HC, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. Arterioscler Thromb Vasc Biol. 1995;15(9):1512-1531. PMID: 7670967
- Nissen SE, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial (REVERSAL). JAMA. 2004;291(9):1071-1080. PMID: 14996776
- Greenland P, et al. ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults. J Am Coll Cardiol. 2010;56(25):e50-e103. PMID: 21144964
- Tabas I, et al. Subendothelial lipoprotein retention as the initiating process in atherosclerosis. Circulation. 2007;116(16):1832-1844. PMID: 17938300
- Virmani R, et al. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 2000;20(5):1262-1275. PMID: 10807742